Irregular Rhythms
March 3, 2013 Leave a comment
-
Sinus Arrhythmia
-
Wandering Pacemaker
-
Atrial Fibrillation

March 3, 2013 Leave a comment
March 3, 2013 Leave a comment
The atria fires an early impulse which causes the heart to beat earlier causing irregularity in the heart rhythm.

The ventricles fire an early impulse which causes the heart to beat earlier causing irregularity in the heart rhythm.

March 3, 2013
Fast rhythms occur when rapid pacing of the heart is coming from an abnormal location (ectopic focus).
Three types of fast rhythms: The keys are the rate and the P waves.
Sudden, rapid rhythms can originate in: atria, AV node (junction), ventricles.
Supraventricular Tachycardia
Both PAT and PJT originate above ventricles and could be called “Supraventricular Tachycardia”





March 2, 2013 Leave a comment
Ischaemia
“Reduced blood flow” – occurs when blood flow to a muscle is insufficient to meet the oxygen requirements of that muscle. When this muscle is the heart, it is termed myocardial ischaemia.
Myocardial ischaemia generally occurs as a result of narrowed coronary arteries. If blood flow is soon increased, or oxygen requirements are lowered, ischaemia will resolve without permanent muscle damage.
Characteristics:
A myocardial infarction (or heart attack) occurs if an adequate blood flow is not restored and the heart muscle dies. Initially symptoms similar to an ischaemic attack will occur as the muscle cells operate anaerobically, however, the pain is sudden and not stress related.

In the following example, the ST segment (shaded) is depressed below the isoelectric PR segment (arrowed).


4 walls of the left ventricle where infractions occur
Lateral infarctions
Inferior infarctions
Anterior Infarctions
February 26, 2013
Characteristics:
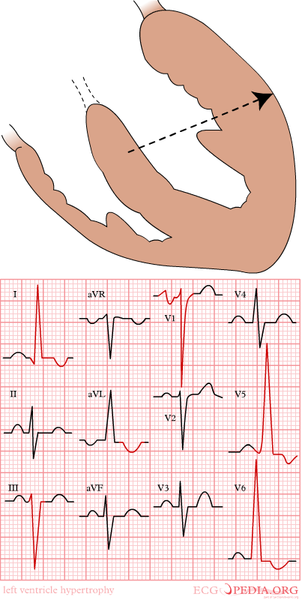
As the left ventricular wall becomes thicker, the QRS complexes become larger.



Right ventricular hypertrophy, the R wave is greater than the S wave in V1
February 26, 2013 Leave a comment
In hypertrophy the heart muscle becomes thicker. Hypertrophy refers to an increase in the size or mass of the heart muscle.
Right atrial enlargement can result from increased pressure in the pulmonary artery, e.g. after pulmonary embolization
Causes:



AKA: Left atrial hypertrophy, left atrial abnormality.
Leads to delayed activation of left atrium and thus prolonged depolarization and a prolonged P wave.
- Left atrial enlargement (LAE) is due to pressure or volume overload of the left atrium.
- It is often a precursor to atrial fibrillation.
LAE produces a broad, bifid P wave in lead II (P mitrale) and enlarges the terminal negative portion of the P wave in V1.
In lead II
- Bifid P wave with > 40 ms between the two peaks
- Total P wave duration > 110 ms
In V1
Characteristics
- A notched P wave in Lead II
- Diagnosed when the second part of the diphasic P wave is biggest.
- Increased duration of the P wave; terminal portion of P wave must span atleast one small box (40 msec)
- P wave with a broad (0.04 sec or 1 small square) and deeply negative (>1 mm) terminal part in V1
- P wave duration longer than 0.12 sec in leads I and / or II (Usually lead II)
Causes
In isolation:
- Classically seen with mitral stenosis
- Left atrial enlargement is also known as “P mitrale” because it is associated with mitral valve insufficiency, resulting in back flow of blood from the left ventricle to the left atrium and subsequent increased local pressure.
In association with left ventricular hypertrophy:
- Systemic hypertension
- Aortic stenosis
- Mitral incompetence
- Hypertrophic cardiomyopathy
Broad (>110ms), bifid P wave in lead II (P mitrale) with > 40ms between the peaks
P wave terminal portion > 40 ms duration in V1

Example 1

Biatrial enlargement due to idiopathic cardiomyopathy:
- Biphasic P waves in V1 with a very tall positive deflection (almost 3 mm in height!) and a negative deflection that is both deep (> 1 mm) and wide (> 40 ms).
Example 2
Biatrial enlargement:
- P waves in lead II are tall (> 2.5mm) and wide (> 120 ms).
- P waves in V2 are tall (> 1.5 mm), while the terminal negative portion of V1 is deep (> 1mm) and wide (> 40 ms).
ECG challenge
Two patients provide an opportunity to apply these principles:
A 75-year-old man with pulmonary hypertension has an ECG as part of his yearly examination (Figure 2; click image to enlarge).

Based on the stepwise approach to evaluating an ECG, consider the following:
(1) Does the ECG indicate a regular heartbeat? Yes, the QRS complexes march out.
(2) Determine the patient’s heart rate by finding a QRS complex on or near a dark line.
Method A: The number of large boxes between Rs is close to four. Four boxes puts the rate at 75 beats per minute.
Method B: Approximately seven QRS complexes occur in 6 seconds (30 large boxes), which estimates the heart rate at 70 beats per minute (7 × 10 = 70).
Method C: Dividing 300 by the number of large boxes between QRS complexes (4) yields an estimate of 75 beats per minute.
(3) A P wave appears before each QRS complex. Is the contour of the P wave the same in all leads? In lead II, the P wave is peaked and has a normal duration. The P wave in V1 is biphasic, with no increase in the upslope of the first deflection.
(4) The PR interval spans approximately three small boxes (0.12 seconds), indicating a sinus rhythm.
(5) The QRS complex spans fewer than three small boxes, which is normal.
(6) The ST segments are neutral, so there is no ischemia.
(7) The T wave is positively deflected in all leads except the aVR.
(8) There are no U waves.
This ECG indicates that the patient is in sinus rhythm and has RAE.
The second patient is a 53-year-old woman who complains of fatigue, dyspnea, and mild chest discomfort. On auscultation, you hear a mid-diastolic low-pitched murmur. The ECG is shown in Figure 3 (click image to enlarge).

(1) Is this ECG regular? Yes, the QRS complexes march out.
(2) Heart rate:
Method A: The number of large boxes between Rs is close to three. Three boxes would put the rate at 100 beats per minute.
Method B: Approximately 10 QRS complexes occur in 6 seconds (30 large boxes), resulting in an estimated rate of 100 beats per minute (10 × 10 = 100).
Method C: Dividing 300 by the number of large boxes between QRS complexes (3) yields a heart rate of 100 beats per minute.
(3) There is a P wave for every QRS complex. Is the contour the same? A notched P wave in lead II has a prolonged duration. The P wave in V1 is biphasic, has an increased down slope in the terminal portion, and spans more than one small box (ie, more than 40 milliseconds in duration).
(4) The PR interval is approximately three small boxes, which is 0.12 seconds, indicating a sinus rhythm.
(5) The QRS complex spans fewer than three small boxes, which is normal.
(6) The ST segments are neutral; there is no ischemia.
(7) The T wave is positively deflected in all leads except the aVR.
(8) There are no U waves.
This ECG indicates that the patient is in sinus rhythm and has LAE.
Sources: JAAPA




